The UPLC™-MS/MS Analysis of Free Thyroxine (FT4) and Free Triiodothyronine (FT3) With a Simplified Equilibrium Dialysis and SPE Workflow for Clinical Research.
Para su uso en investigación únicamente. No se debe utilizar para procedimientos de diagnóstico.
Abstract
This application note demonstrates a simple equilibrium dialysis, SPE, and data analysis workflow for the analysis of free thyroxine (FT4) and free triiodothyronine (FT3) in human serum within a typical working day for clinical research.
Benefits
- Simplified Equilibrium Dialysis, SPE and Data Analysis workflow that can be performed within a typical working day
- Reduced LC-MS runtime to allow for a large number of samples to be processed
- Chromatographic resolution of T3 and Reverse T3
- Low analytical sensitivity levels utilizing the Xevo™ TQ Absolute Mass Spectrometer
Introduction
Thyroid stimulating hormone (TSH) is produced by the pituitary gland and the amount of TSH regulates production of the thyroid hormones Thyroxine (T4) and Triiodothyronine (T3). In circulation, approximately 99.98% of T4 and 99.7% of T3 is bound to transport proteins, with the remaining portion being free (FT4 and FT3, respectively) and biologically active.
Measurement of FT4 and FT3 is typically performed by immunoassay, however these can be prone to suffer from interferences and a lack of specificity. Currently, the accepted gold standard for the measurement of FT4 and FT3 is using equilibrium dialysis (ED) and combined with the use of LC-MS/MS can overcome the issues with immunoassay in the measurement of FT4 and FT3. However, the equilibrium dialysis procedure can be quite time consuming and often being performed overnight.
Here, we describe a simple clinical research method to perform ED using a commercially available device followed by sample preparation by solid phase extraction (SPE) and UPLC-MS/MS analysis using the Waters™ ACQUITY™ UPLC and analytically sensitive Xevo TQ Absolute Mass Spectrometer for clinical research. Data analysis and review has been simplified with the use of the waters_connect™ with QUAN Review Software. This has allowed for the complete workflow including equilibrium dialysis to be performed within a typical working day.
 Figure 1. The ACQUITY UPLC I-Class FL and Xevo TQ-Absolute Mass Spectrometer.
Figure 1. The ACQUITY UPLC I-Class FL and Xevo TQ-Absolute Mass Spectrometer.
Experimental
Sample Preparation
Thyroxine (T4), Triiodothyronine (T3), [13C6]-Thyroxine and [13C6]-Triiodothyronine certified reference solutions were purchased from Merck Life Sciences (Gillingham, UK). LCMS Grade methanol, LCMS Grade water and LCMS Grade 2-propanol were obtained from Honeywell (Fisher Scientific, Loughborough, UK). LCMS Grade acetonitrile was obtained from Biosolve (Dieuze, France). Ammonia (28%) was obtained from VWR (Lutterworth, UK). Sodium chloride, potassium phosphate, potassium chloride, magnesium sulphate, urea, sodium azide, calcium chloride, and 1 M HEPES buffer were all purchased from Merck Life Sciences (Gillingham, UK). Human serum, both pooled and individual samples were obtained from BioIVT (West Sussex, UK). CDC Phase 1 samples were obtained from the Centers for Disease Control and Prevention (Atlanta, USA) and UK NEQAS samples were obtained from the National External Quality Assurance Scheme (Birmingham, UK) for method comparison studies.
Calibrators were prepared in dialysate buffer across the following concentration ranges (Table 1), with Quality Control (QC) concentrations being shown in round brackets. These Calibrators and QCs were not dialyzed through the ED process but were extracted using the SPE procedure. Serum QC samples were also processed during precision runs (from an individual sample), which were dialyzed and extracted. These samples were value assigned using the method and are shown in square brackets.
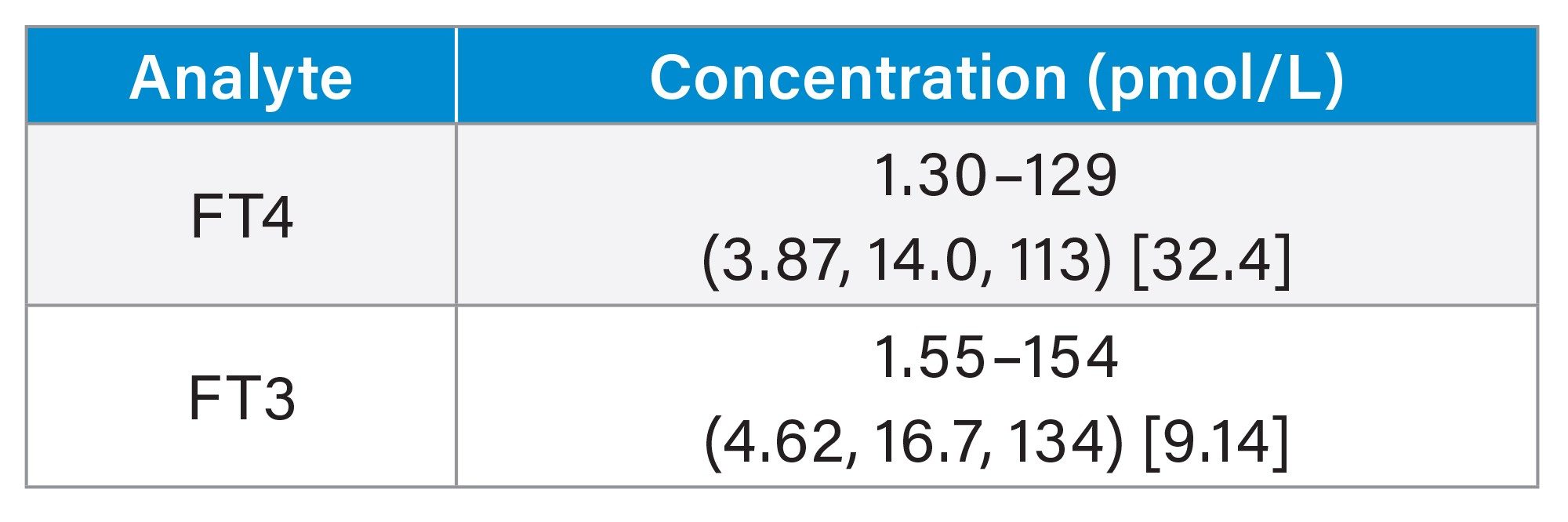 Table 1. Calibration Range and QC Values for FT4 and FT3.
Table 1. Calibration Range and QC Values for FT4 and FT3.
Equilibrium Dialysis (ED) Procedure
ED was not performed on the calibrators or spiked QCs. These samples were extracted directly from the dialysate buffer.
- 200 µL of serum sample was added to the sample chamber of the ED device
- 400 µL of HEPES buffer was added to the dialysate chamber of the ED device
- Samples were mixed at 37 °C until equilibrium had been reached
- The ED inserts were removed and Internal Standard working solution was added and mixed thoroughly
- Sample Diluent was added, and the plate was mixed thoroughly
- Samples were transferred directly to the pre-conditioned SPE plate and the SPE procedure is followed
Calibrator/Spiked QC and non ED Samples Procedure
- 300 µL of calibrator/spiked QC were prepared across the concentration ranges shown above in microfuge tubes
- Internal Standard working solution was added to calibrators/QCs and non ED samples mixed thoroughly
- Sample Diluent was added, and samples were mixed thoroughly
SPE Procedure
- An Oasis™ MAX µElution™ plate was pre-conditioned using methanol followed by water
- All samples (calibrator, QC, non-ED, and ED samples) were transferred (complete volume) and drawn through the plate
- Samples were washed thoroughly with a basic solution followed by water and then a mixture of methanol and acetonitrile
- LCMS Grade water was added to a 700 µL round well collection plate and this was placed beneath the SPE plate
- Samples were eluted using 2 aliquots of Elution Solution in acid and the collection plate was sealed and mixed thoroughly prior to injection
LC Conditions
|
LC system: |
ACQUITY UPLC I-Class FL with Column Manager |
|
Column(s): |
ACQUITY Premier HSS T3, 1.8 µm VanGuard™ FIT, 2.1 x 50 mm |
|
Column temperature: |
45 ˚C ± 2 ˚C |
|
Sample temperature: |
8 ˚C |
|
Injection volume: |
35 µL |
|
Mobile phase A: |
LCMS Grade water with 0.1% formic acid |
|
Mobile phase B: |
50/50 (v/v) LCMS Grade methanol / LCMS Grade acetonitrile with 0.1% formic acid |
|
Runtime: |
2.5 min (injection to injection time of approx. 3.5 min) |
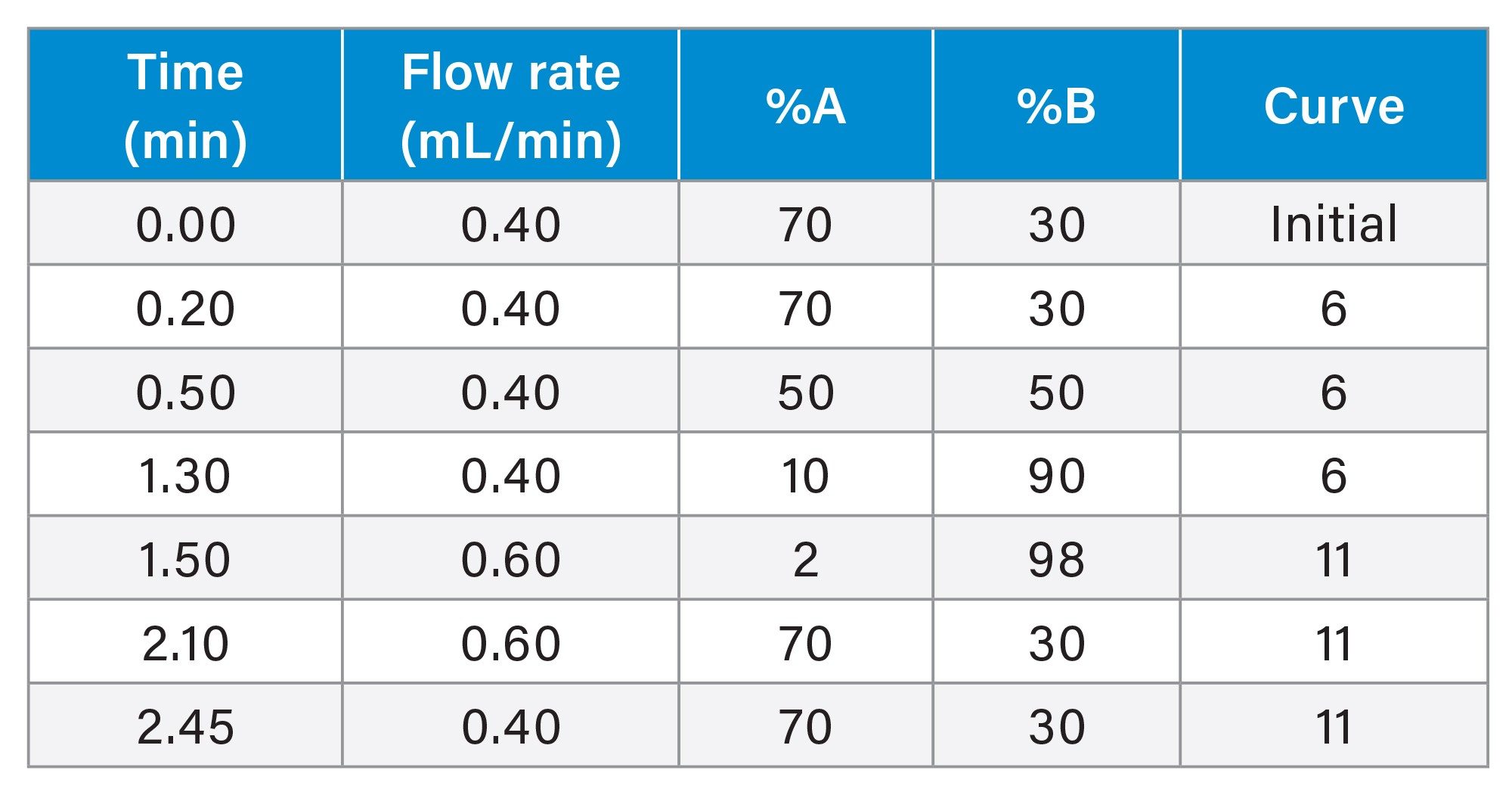
Gradient Table
MS Conditions
|
MS system: |
Xevo TQ Absolute |
|
Ionization mode: |
Positive electrospray ionization |
|
Capillary voltage: |
3.0 kV |
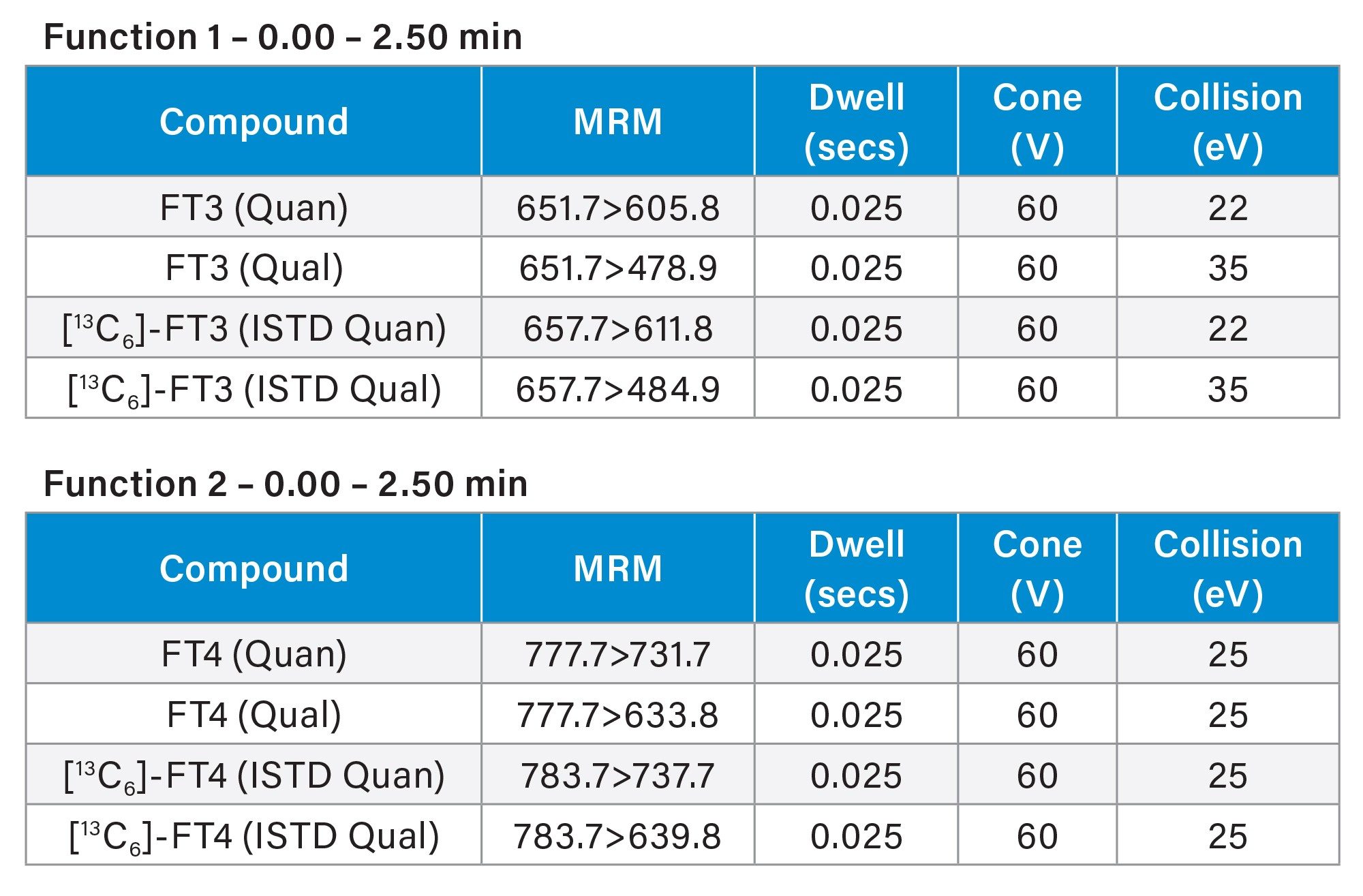
MRM Method
Data Analysis
Data analysis was performed using waters_connect with QUAN Review Software (Figure 2).
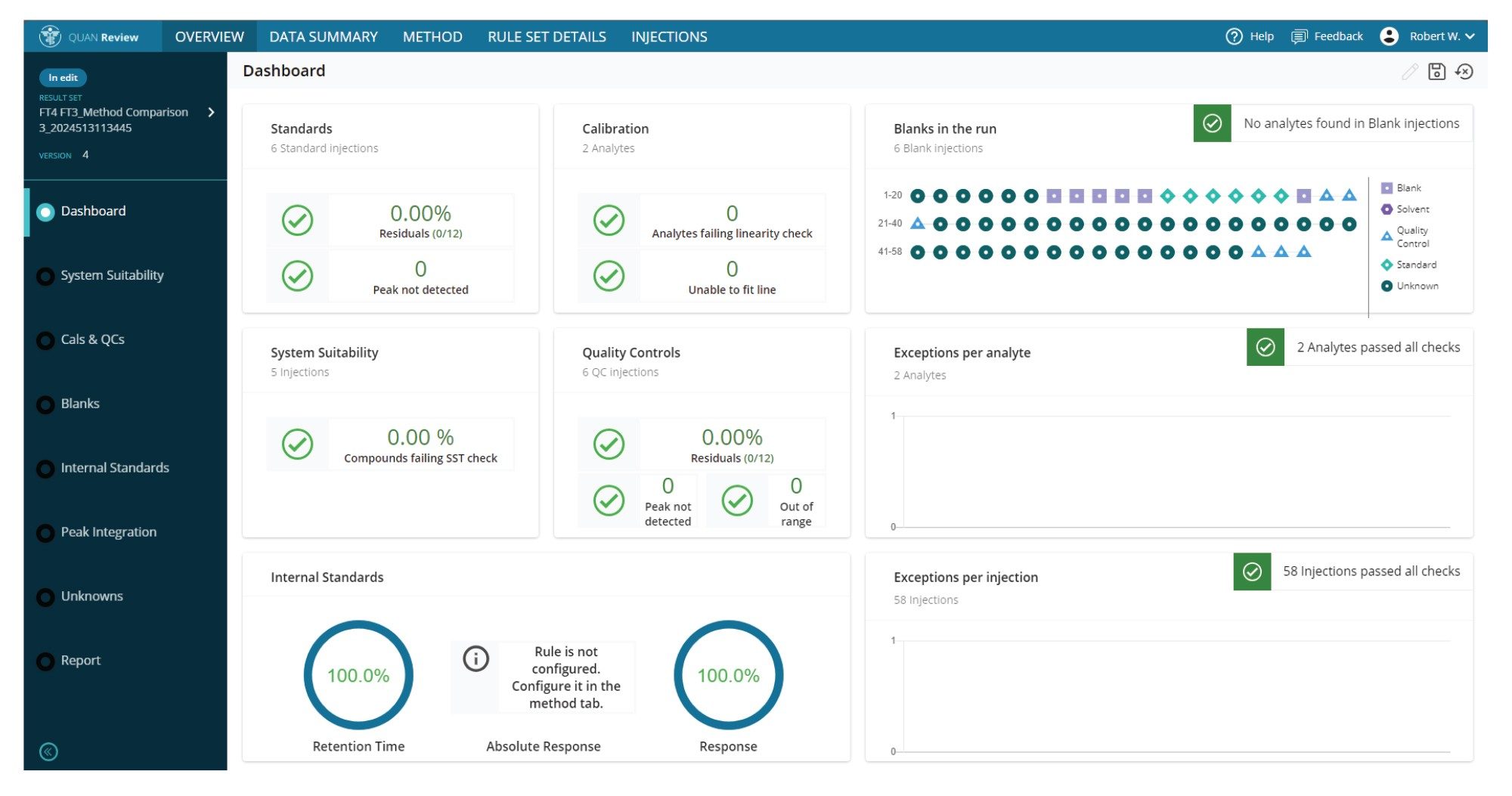 Figure 2. QUAN Review overview tab for a FT4 and FT3 data processing run.
Figure 2. QUAN Review overview tab for a FT4 and FT3 data processing run.
Results and Discussion
Below are example chromatograms of FT4 and FT3 from human serum samples which have been dialyzed, extracted and analyzed (Figure 3) and then data analysis performed in QUAN Review. Calculated concentrations of the samples were 4.95 pmol/L for FT4 and 7.12 pmol/L for FT3. Reverse FT3 is also separated from FT3 to prevent interference.
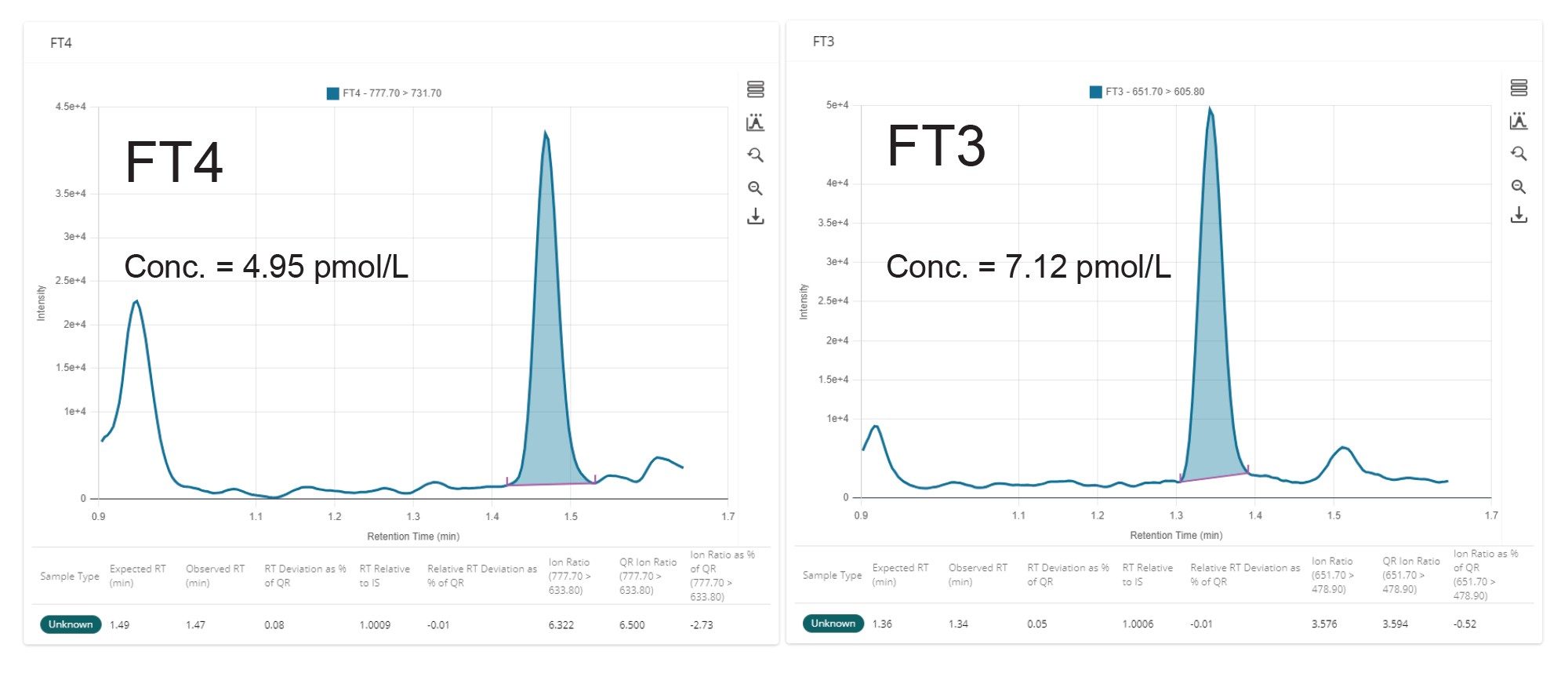 Figure 3. Typical Chromatograms of FT4 and FT3 from human serum samples which have been dialyzed, extracted, and analyzed.
Figure 3. Typical Chromatograms of FT4 and FT3 from human serum samples which have been dialyzed, extracted, and analyzed.
Precision of both QC samples in dialysate that had just gone through the extraction process and also serum QC samples that had been dialyzed and then extracted were assessed. This was performed by extracting and measuring five replicates of the QC L, QC M, QC H, and the serum QC across five occasions. Data was processed and statistical analysis performed using Analyse-it in Excel. Within-run and total precision were ≤5.0% CV for the dialysate QC samples and ≤9.6% CV for the serum QC samples across all concentration levels for both FT4 and FT3 as shown in Table 2.
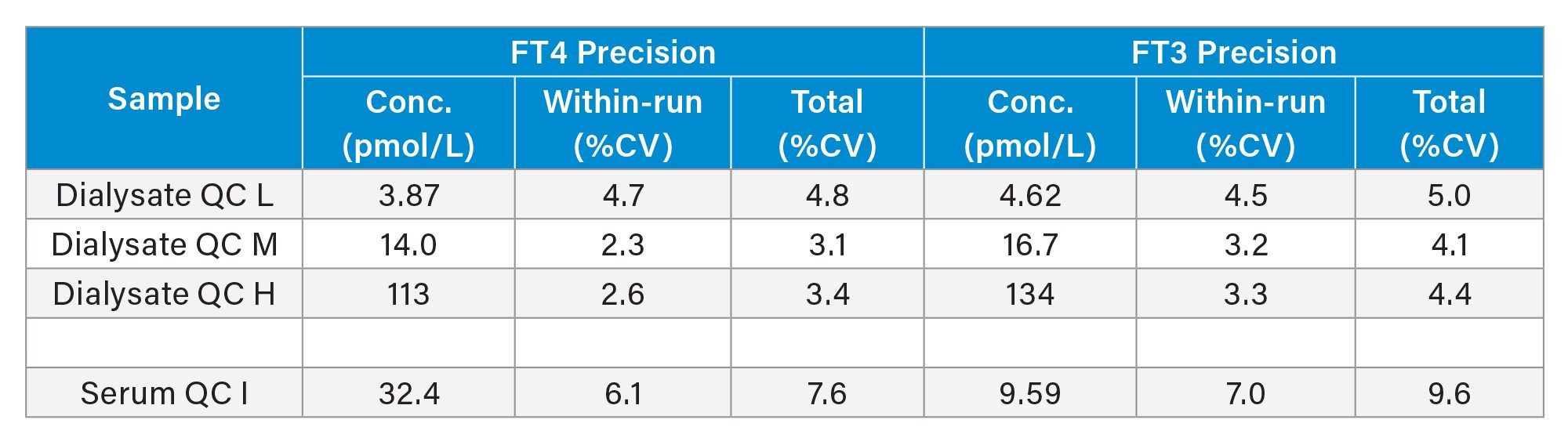 Table 2. Precision Performance Summary for FT4 and FT3.
Table 2. Precision Performance Summary for FT4 and FT3.
Analytical sensitivity of the method was assessed by extracting and analyzing 10 replicates of dialysate buffer spiked at low concentration levels over five occasions. The Lower Limit of Quantification (LLoQ) was determined to be the lowest concentration at which precision was ≤20% CV and signal to noise ratio (S:N) was >10:1 peak to peak (ptp). The LLoQ for FT4 and FT3 were determined to be 0.97 pmol/L and 1.15 pmol/L respectively, with chromatograms of an LLoQ sample being shown in Figure 4.
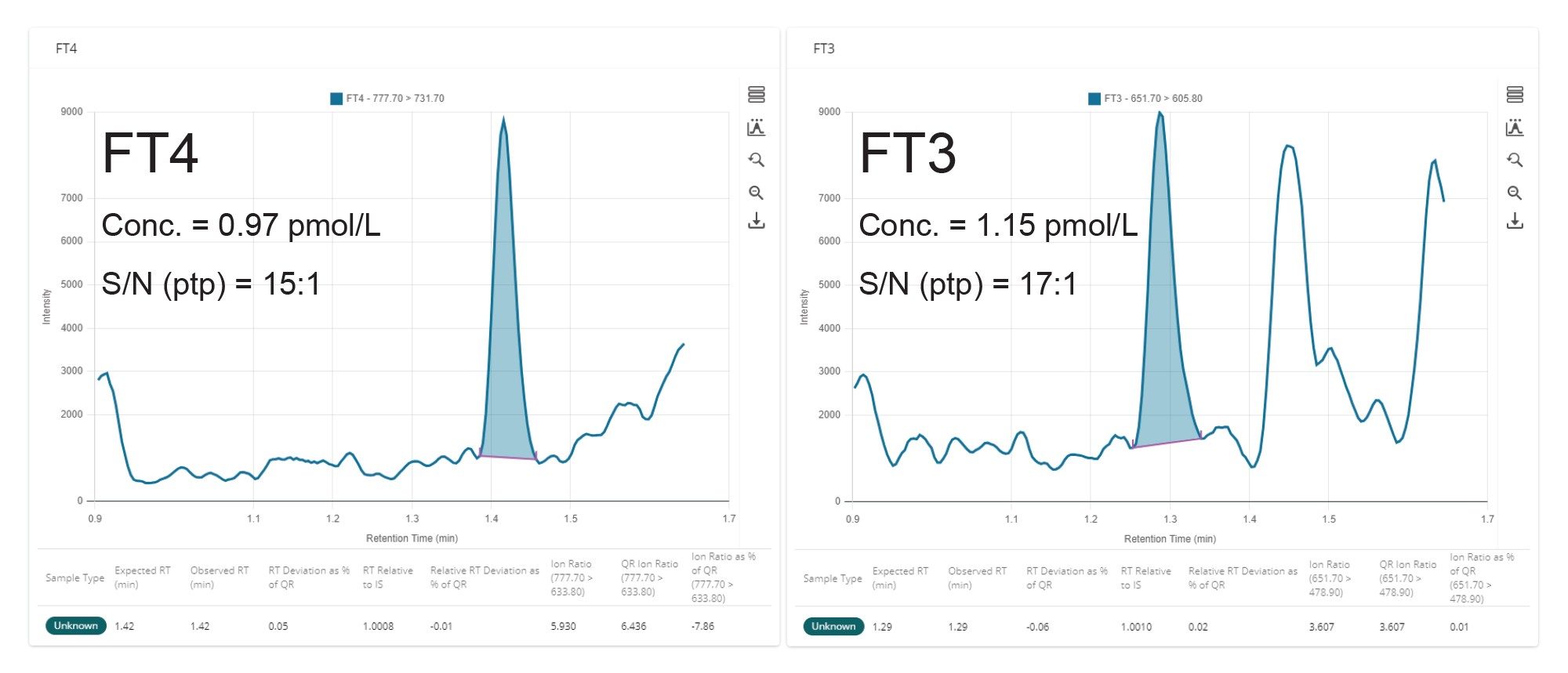 Figure 4. Typical chromatograms of FT4 and FT3 spiked in dialysate, extracted, and analyzed.
Figure 4. Typical chromatograms of FT4 and FT3 spiked in dialysate, extracted, and analyzed.
Linearity was assessed as described in CLSI EP06-Ed02 where dialysate buffer was spiked at a high and low concentration of T4 and T3 and these were mixed in known ratios covering the calibration range. The 4 aliquots were taken from each of the 11 concentration levels, extracted and analyzed. Data was processed and statistical analysis was performed using Analyse-it in Excel. Samples were shown to be linear from 1.11–177 pmol/L for FT4 and 1.32–211 pmol/L for FT3, having an allowable non-linearity of ±10%, giving a large analytical range due to sample dilution not being possible (Figure 5).
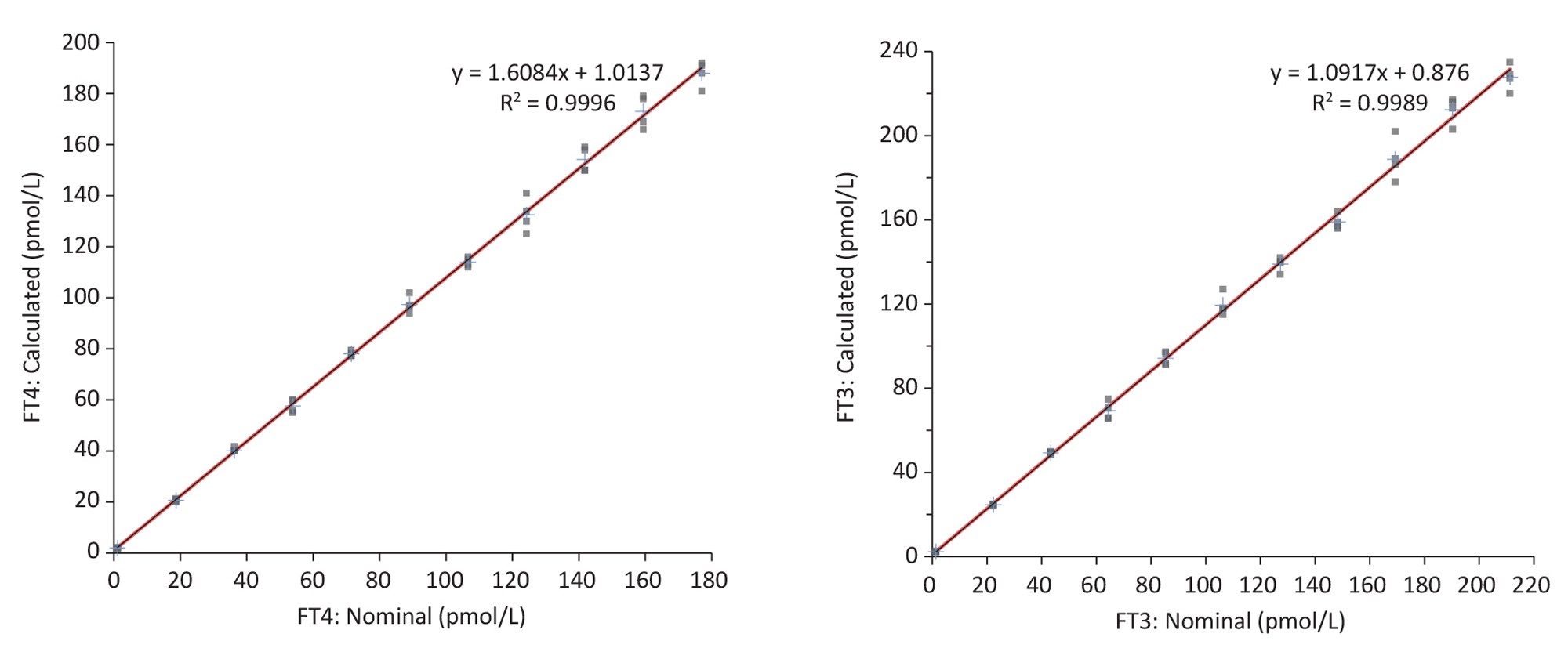 Figure 5. Linearity test results for FT4 and FT3.
Figure 5. Linearity test results for FT4 and FT3.
Further to this, all calibration lines performed during testing were linear, having a coefficient of determination (r2) of >0.995 and percentage deviations of within ±15% (±20% for Cal 1) for both FT4 and FT3
Carryover of the method was assessed by analyzing a series of extracted high samples (spiked dialysate at 258 pmol/L and 308 pmol/L) for FT4 and FT3 followed by blank (dialysate). No significant carryover was observed, with the calculated mean peak areas being <20% of the Calibrator 1 sample. Consistent recovery was achieved, comparing pre- and post-spiked samples at low and high concentration levels.
Typical endogenous interferences (albumin, bilirubin, cholesterol, intralipid, triglycerides and uric acid) were tested and percentage recoveries of the test samples compared to controls were all within ±12.4%. Matrix effect investigations were performed by performing ED on 10 replicates of MSG4000 stripped human serum. These samples were then extracted and then five replicates were spiked at a low concentration and five replicates were spiked at a high concentration. 10 replicates of dialysate buffer were also extracted and then 5 replicates spiked at a low concentration and five replicates were spiked at a high concentration. Control samples were prepared by spiking elution solvent at low and high concentrations. Matrix Factor results are shown in Table 3. Little to no suppression was observed when comparing Dialysate test samples to controls for peak area and internal standard response ratio for both FT4 and FT3. Some suppression was observed when comparing serum test samples to controls for peak area, but suppression effects were compensated for by the internal standard and response ratios were within ±15% for both FT4 and FT3.
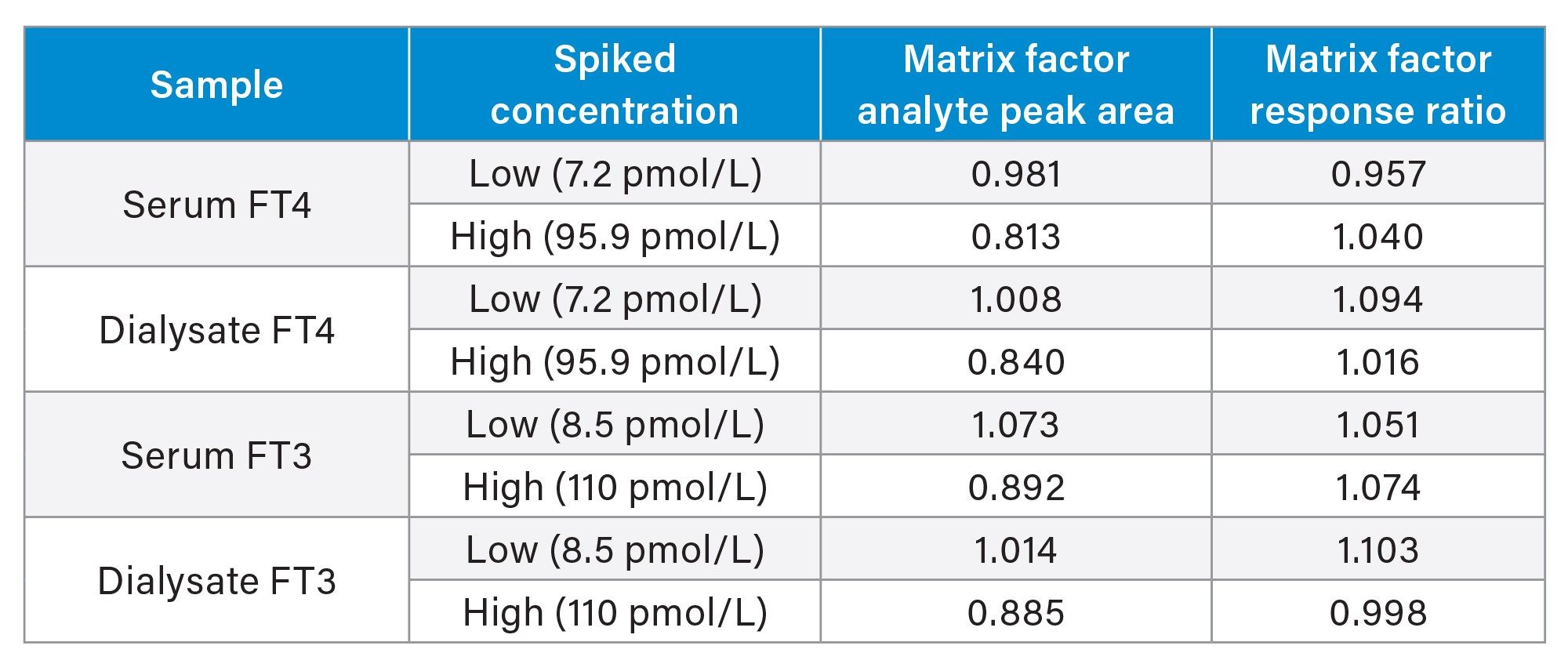 Table 3. Matrix Effects Summary for FT4 and FT3.
Table 3. Matrix Effects Summary for FT4 and FT3.
Following value assignment of our calibrators, method comparison was performed by performing equilibrium dialysis, sample extraction and LC-MS/MS analysis of 40 serum samples received from the CDC HoSt Phase 1 Program for FT4 and comparing the Waters results to the reference measurement procedure values. A Passing-Bablok fit of y=0.9198x + 1.243 (Figure 6) and a Bland Altman bias of 0.070% was obtained when performing statistical analysis of the data using Analyse-it in Excel.
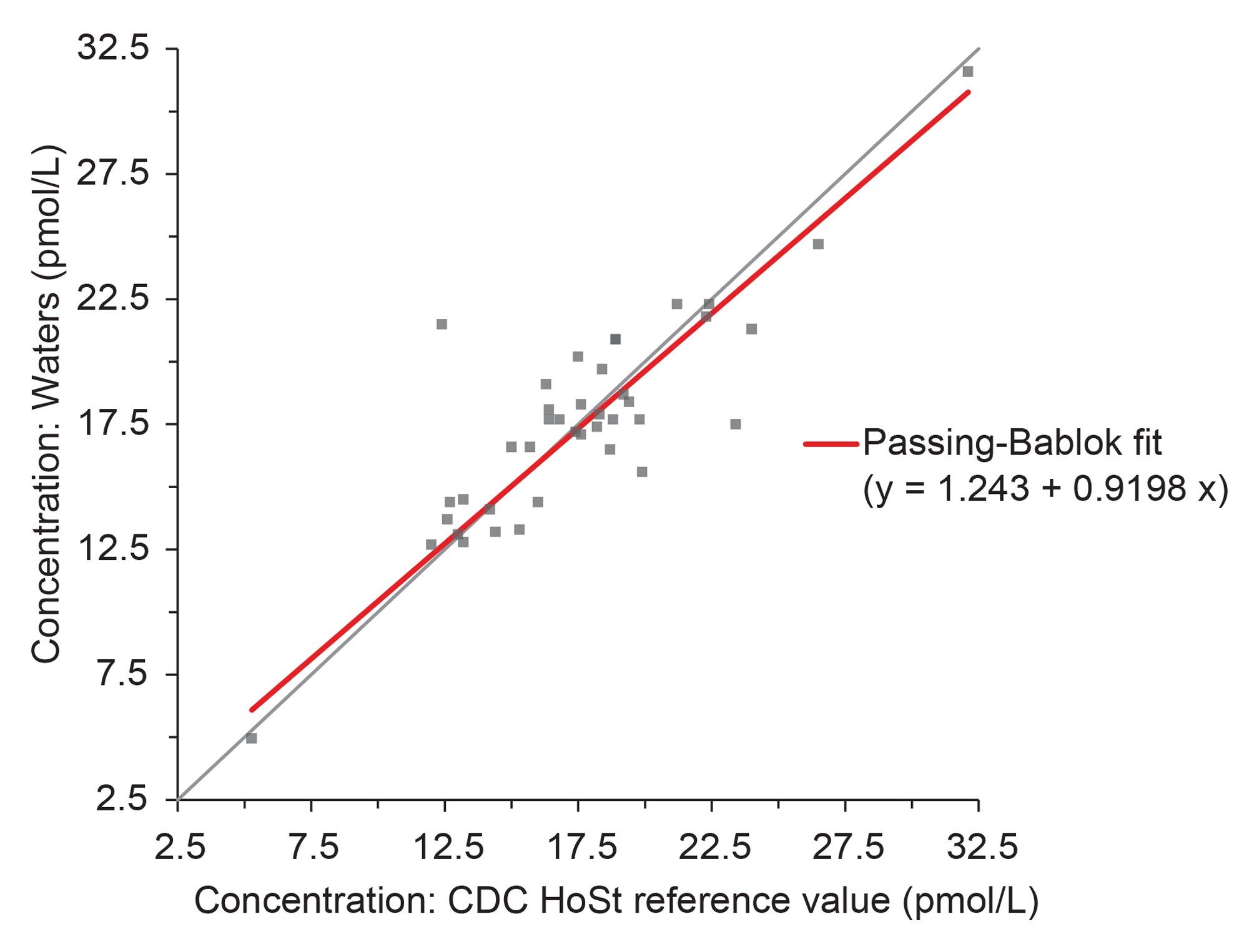 Figure 6. Passing-Bablok fit for FT4, comparing our method to the CDC HoSt reference measurement procedure.
Figure 6. Passing-Bablok fit for FT4, comparing our method to the CDC HoSt reference measurement procedure.
We also compared our method to the UK NEQAS scheme, where results from our method were compared against the ALTM values, which were derived from immunoassay methods (Figure 7). We observed a high bias when comparing to these values, similar to that published by the reference measurement procedure at the University of Ghent when comparing to different immunoassay methods.1 A similar trend was also observed for FT3 when comparing to the UK NEQAS ALTM values (Figure 8).
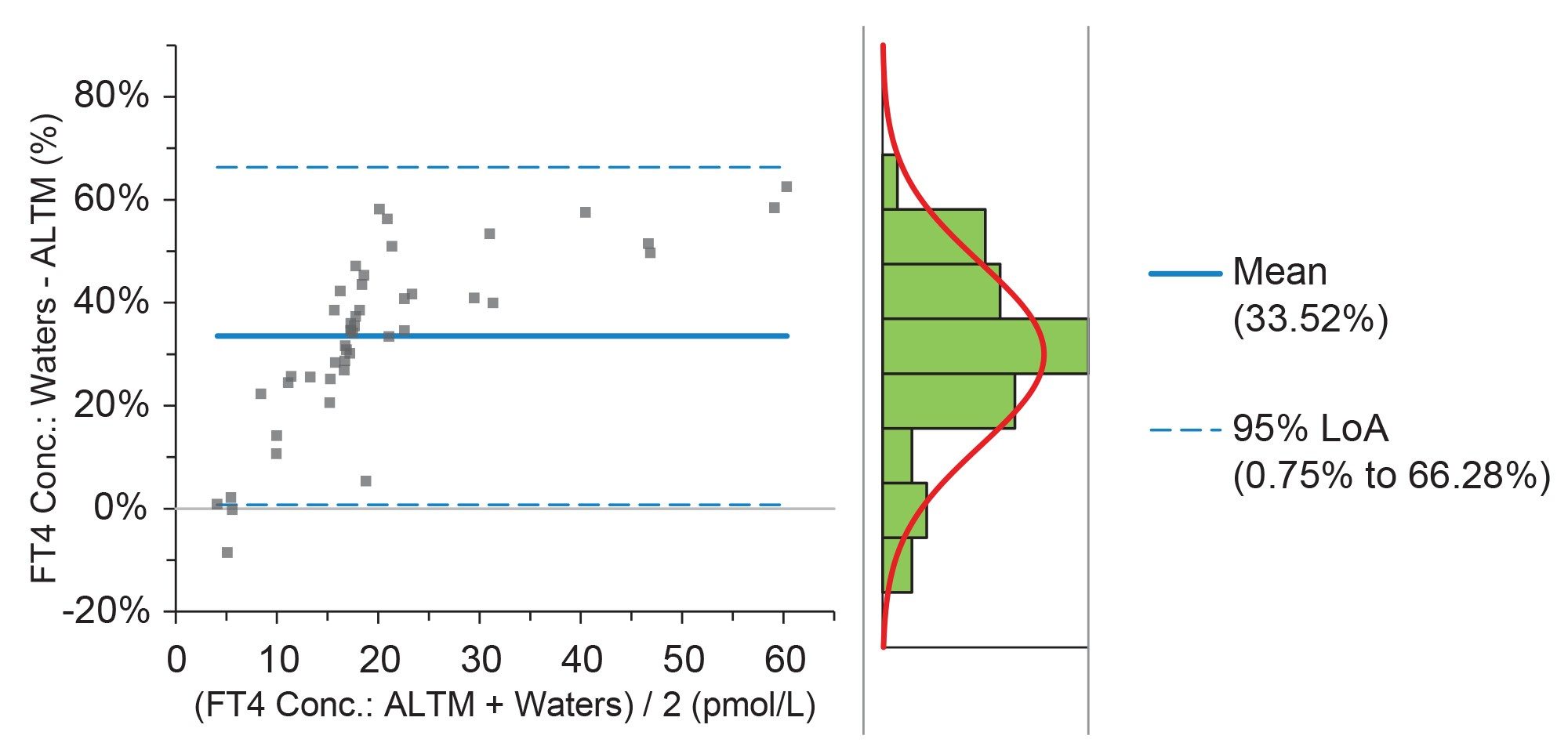 Figure 7. Bland-Altman Comparison of the UK NEQAS Scheme ALTM Vs our method for FT4.
Figure 7. Bland-Altman Comparison of the UK NEQAS Scheme ALTM Vs our method for FT4.
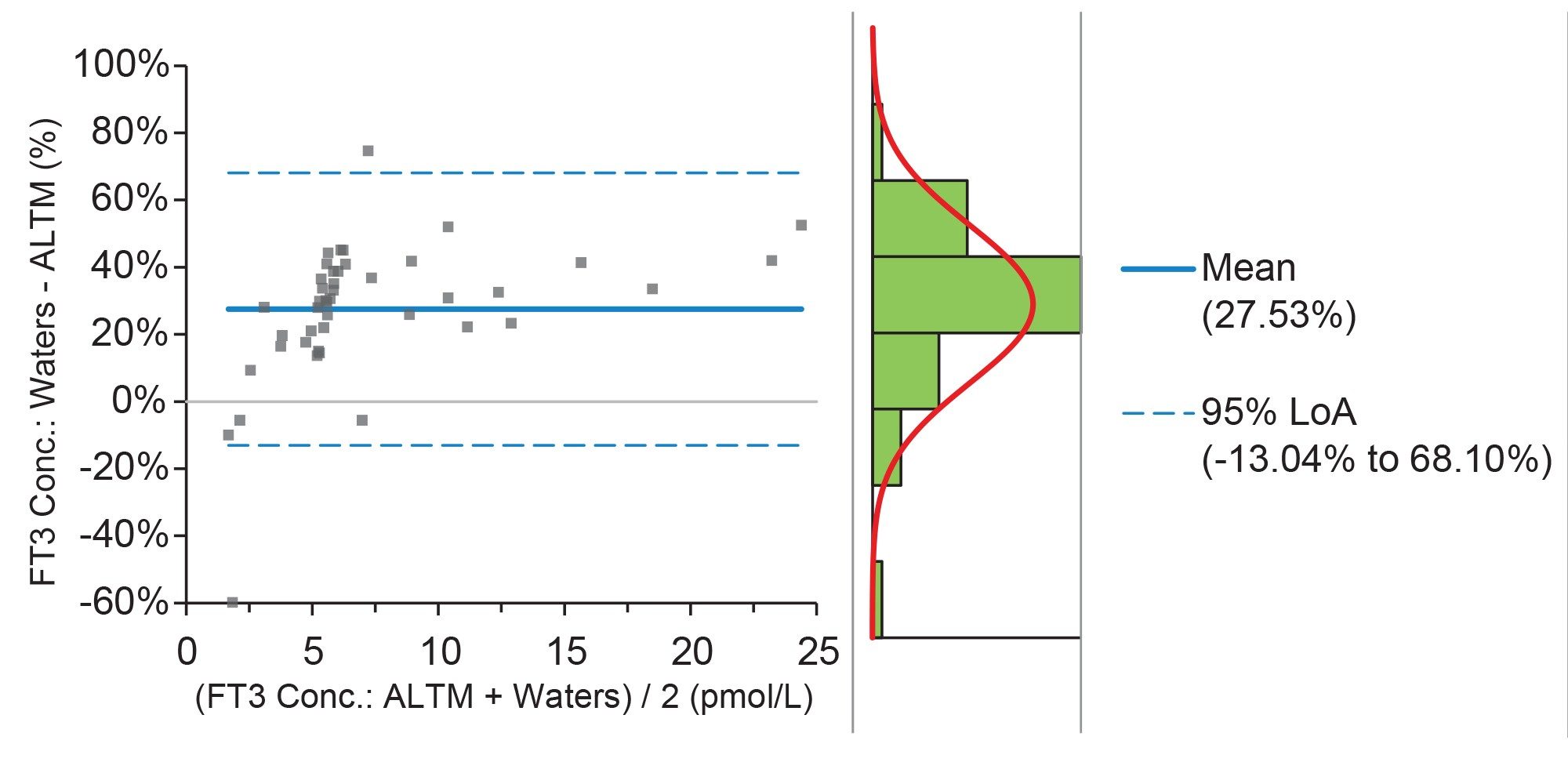 Figure 8. Bland-Altman Comparison of the UK NEQAS Scheme ALTM Vs our method for FT3.
Figure 8. Bland-Altman Comparison of the UK NEQAS Scheme ALTM Vs our method for FT3.
Conclusion
A clinical research method has been developed for the UPLC-MS/MS analysis of Free Thyroxine (FT4) and Free Triiodothyronine (FT3) from human serum using a simple equilibrium dialysis and SPE procedure which can be completed within a typical working day. Data analysis was also simplified using the waters_connect with QUAN Review Software. The method was shown to have excellent precision, analytical sensitivity and method comparison results to the CDC HoSt reference measurement procedure.
- Calibration curves had correlation coefficients (r2) of >0.995 for all runs for FT4 and FT3
- Within-run and total precision results for FT4 were ≤4.8% CV across all concentrations tested for spiked dialysate QC samples and ≤7.6% for dialyzed and extracted serum samples. For FT3, the precision results were ≤5.0% and 9.6% CV, respectively
- Analytical sensitivity concentrations of 0.97pmol/L for FT4 and 1.15pmol/L for FT3, having a %CV of ≤20% and S:N (ptp) of >10:1
- Little to no ion suppression was observed when comparing internal standard response ratios to control samples
- The method has shown to be comparable to the CDC HoSt Phase 1 program, comparing well to the reference measurement procedure, having a Passing-Bablok fit of y=0.9198x + 1.243 and a Bland Altman bias of 0.070% for FT4
References
- De Grande L, Van Uytfanghe K, Reynders D, Das B, Faix J, MacKenzie F, Decallonne B, Hishinuma A, Lapauw B, Taelman P, Van Crombrugge P, Van den Bruel A, Velkeniers B, Williams P and Thienpont L on behalf of the IFCC Committee for Standardization of Thyroid Function Tests (C-STFT). Standardization of Free Thyroxine Measurements Allows the Adoption of a More Uniform Reference Interval. Clinical Chemistry. 2017 October; 63:10; Pages 1585–1593.
Acknowledgement
We would like to thank Katleen Van Uyfanghe for her support during method development.
720008453, August 2024